The Insulin Lock: How Eating Three Times a Day Traps Fat Inside Your Body
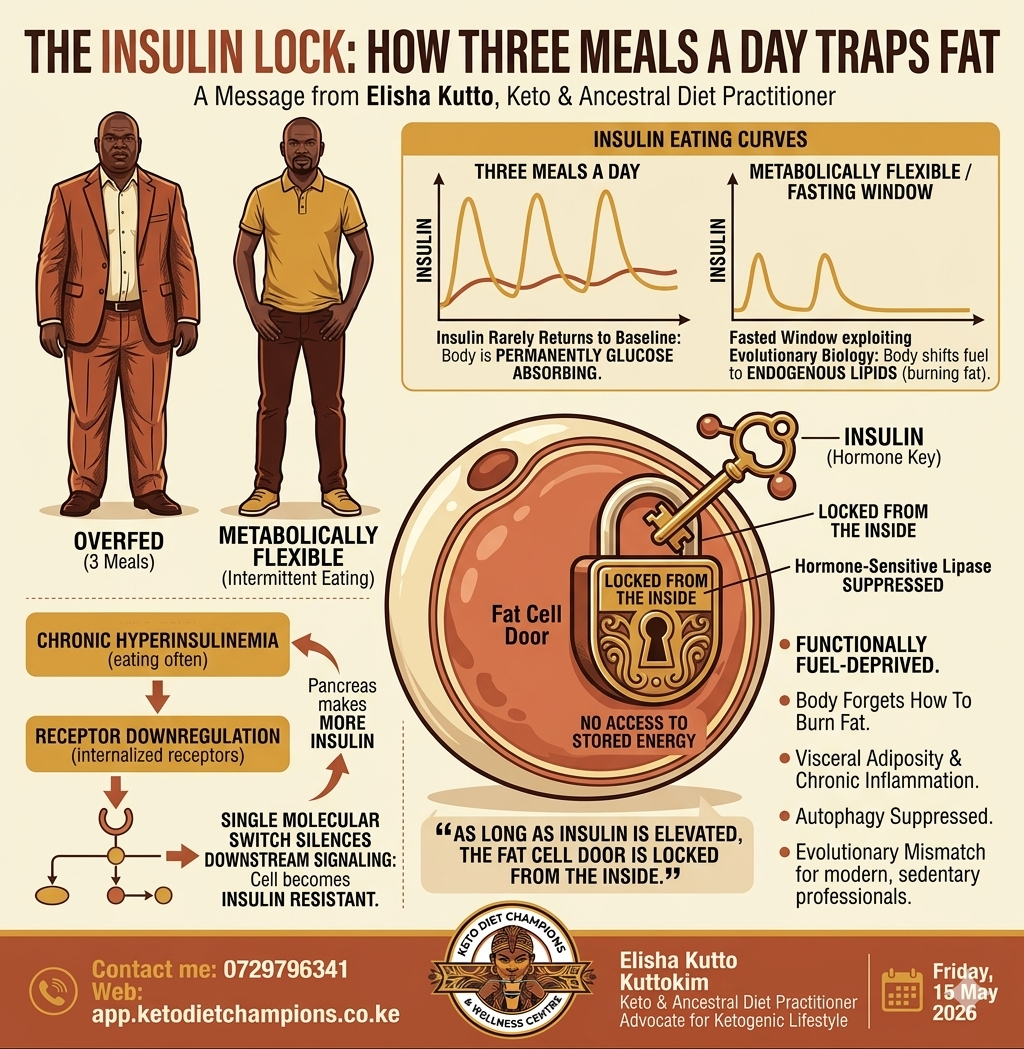
In plain terms: as long as insulin is elevated, the fat cell door is locked from the inside. The body cannot access its own stored energy reserves, regardless of how much adipose tissue has accumulated
Elisha Kutto
Friday, 15 May 2026
Why Three Meals a Day Is Making Us Fat: The Insulin Story Nobody Tells You
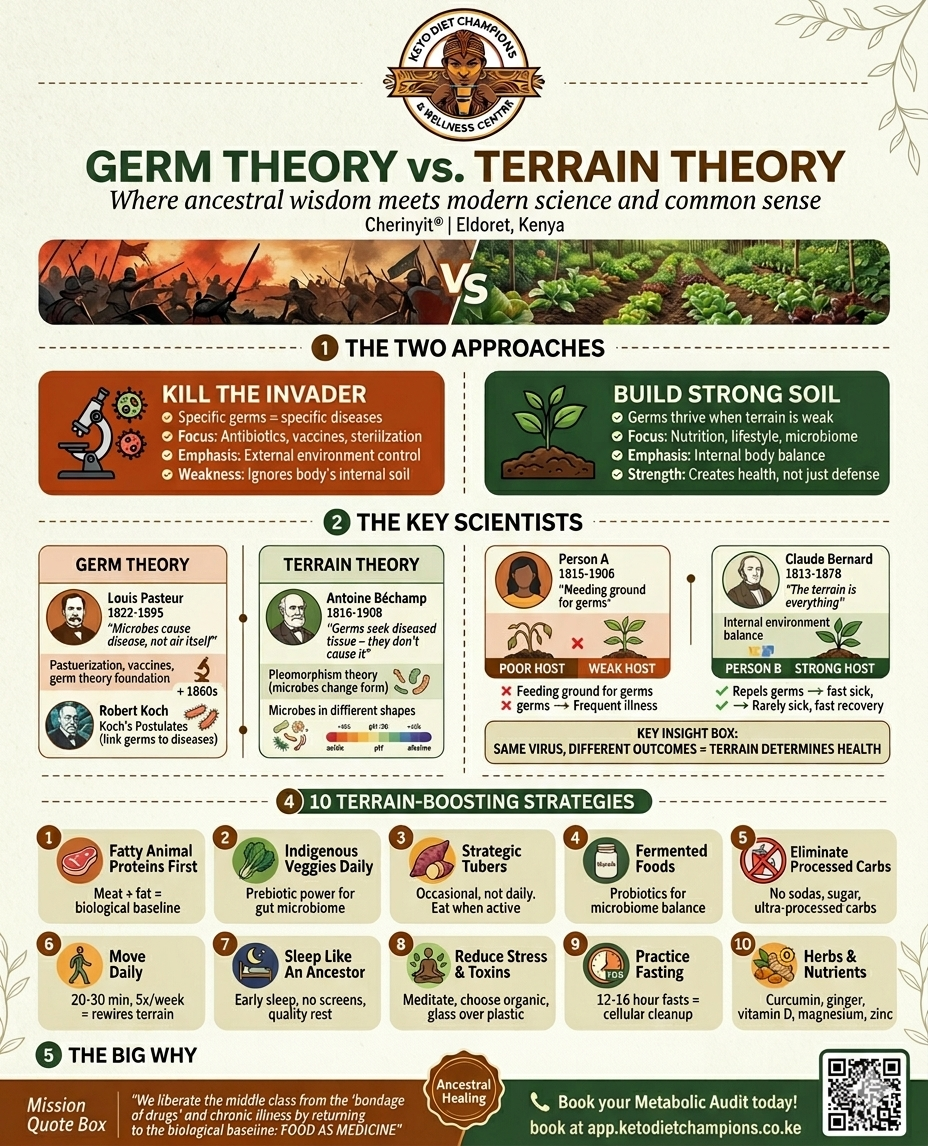
If I were to identify one dietary habit that has silently engineered the modern metabolic crisis, it would not be sugar alone, nor sedentary living in isolation — it would be the unquestioned ritual of eating three times a day, every day, without pause. This seemingly innocent schedule has become one of the most underappreciated drivers of weight gain, insulin resistance, and ultimately, type 2 diabetes.
The Insulin Trap: A Hormone that Never Rests Every time we eat — regardless of what we eat — the pancreas responds by secreting insulin, the primary anabolic hormone responsible for shuttling glucose from the bloodstream into cells. In a metabolically healthy individual, insulin rises sharply after a meal, facilitates cellular glucose uptake, and then gradually returns to a low baseline during the inter-meal fasted state. It is during this fasted window that the body shifts its fuel preference from exogenous glucose to endogenous lipids — a physiological transition known as metabolic flexibility
The problem with a strict breakfast-lunch-dinner structure, particularly in a modern food environment where over 40% of dietary calories are derived from refined carbohydrates and ultra-processed foods, is that insulin levels rarely complete this return to baseline. By the time the post-prandial insulin curve from lunch begins to descend, dinner is already being prepared. The body effectively exists in a state of permanent glucose absorption — what physiologists call the post-prandial state — never entering the fasted, fat-oxidizing phase that our evolutionary biology was designed to exploit
How Chronic Hyperinsulinemia Locks the Fat Cell: Insulin is, at its biochemical core, a storage hormone. Its presence in circulation activates lipoprotein lipase on adipocyte membranes while simultaneously suppressing hormone-sensitive lipase — the very enzyme responsible for liberating stored triglycerides for oxidation. In plain terms: as long as insulin is elevated, the fat cell door is locked from the inside. The body cannot access its own stored energy reserves, regardless of how much adipose tissue has accumulated.This is the metabolic paradox I observe repeatedly in my wellness practice in Eldoret: individuals who are overfed yet functionally fuel-deprived, caught in a cycle where the persistent hormonal signal to store energy makes meaningful fat oxidation nearly impossible without deliberate dietary restructuring.
The Molecular Pathway to Insulin Resistance: When the pancreas is compelled to secrete insulin repeatedly throughout the day — particularly in response to high-glycaemic carbohydrate loads — the target tissues, primarily skeletal muscle, hepatocytes, and adipocytes, begin to defend themselves through a process of receptor downregulation. Chronic exposure to supraphysiological insulin concentrations triggers the internalization and degradation of insulin receptors on the cell surface, reducing the density of available binding sites. Simultaneously, intracellular insulin signaling is disrupted at the level of insulin receptor substrate-1 (IRS-1). Excess circulating free fatty acids and diacylglycerol — byproducts of perpetual lipid overflow from overfilled adipocytes — activate serine kinases such as protein kinase C (PKC) and c-Jun N-terminal kinase (JNK), which phosphorylate IRS-1 at serine residues rather than tyrosine residues. This single molecular switch effectively silences the downstream signaling cascade — blocking the translocation of GLUT4 glucose transporters to the cell surface and preventing glucose uptake. The cell becomes, by every functional definition,insulin resistant.The pancreatic beta cells respond to rising blood glucose by secreting even more insulin, accelerating a compensatory hyperinsulinaemic state that perpetuates the very receptor downregulation it seeks to overcome. This self-reinforcing cycle is the biochemical engine behind the transition from normal glucose tolerance to prediabetes and eventually overt type 2 diabetes mellitus.
From Metabolic Inflexibility to Chronic Disease: As insulin sensitivity erodes progressively, the body loses its enzymatic efficiency to mobilize and oxidize stored fat. The mitochondrial machinery responsible for beta-oxidation — including carnitine palmitoyltransferase I (CPT-1), the rate-limiting enzyme for fatty acid entry into the mitochondrion — becomes functionally suppressed in the context of chronic carbohydrate surplus and hyperinsulinaemia (Muoio, 2014). The body, effectively forgets how to burn fat, becoming entirely dependent on the next bolus of exogenous glucose to maintain energy homeostasis.This persistent hormonal dysregulation does not confine its damage to glycaemic control alone. Chronic hyperinsulinaemia drives hepatic de novo lipogenesis, elevating circulating triglycerides and promoting visceral adiposity — the metabolically active fat depot most strongly associated with systemic inflammation and cardiovascular risk. It simultaneously suppresses autophagy, the critical intracellular housekeeping process by which the body identifies, dismantles, and recycles damaged proteins and dysfunctional organelles. When mTOR remains chronically activated by persistent insulin signaling, autophagic flux is inhibited, accelerating cellular senescence and the inflammatory milieu that underpins metabolic syndrome.
The Evolutionary Mismatch and the Modern African Context:The three-meal schedule was, in historical context, designed for populations engaged in sustained manual labor — individuals whose daily energy expenditure was sufficient to create meaningful caloric deficits between meals. For the modern professional in any urban African city, who spends the majority of their working hours seated and commutes by vehicle, this model represents a profound biological mismatch. The human cost of this mismatch daily — rising rates of visceral obesity, hypertension, and type 2 diabetes that are no longer diseases of affluence but diseases of dietary pattern.
KuttoKim- Keto & Ancestral Diet Practitioner/Advocate for Ketogenic Lifestyle
Ready to Start?
Book a consultation today
Take the first step toward your health transformation with a KSh 300 consultation.
Book Now →